A Brief History of the SARS-CoV-2 Coronavirus Pandemic From the Body Scientific Columns of the Lakeville Journal and The Berkshire Edge
During the Covid-19 epidemic, I wrote 12 columns on the virus for The Lakeville Journal, The Berkshire Edge, and Norfolk Now. The field moved from a few scientific papers in January 2020 to tens of thousands now. The deliberate pace of science became too slow, and papers appeared on special servers prior to peer review to speed research. Information changed from week to week as experiments were done and clinical trials were completed. We learned a lot about how the virus works, how to treat it, and how not to treat it. Vaccines were made and tested. Mutants of SARS-CoV-2 appeared, as expected, but the ability of these viruses to evolve so quickly was a surprise. The methods to create the new vaccines were novel—the mRNA vaccines of Moderna and Pfizer and several other vaccines have advantages over traditional methods, which take much longer. A complete vaccine treatment with boosters protects against hospitalization and death from known mutant forms of SARS-CoV-2, except in rare cases. A new vaccine containing the Omicron variants is available (September 2022). Long Covid is still a misery and a bit of a mystery, but it is coming into focus, with a great deal of money appropriated to study it. No pandemic passes without the intervention politics and controversy, but in the end, the vaccines saved 20 million lives and counting.
This essay is my effort to integrate the columns. It was not easy because questions in February 2020 were answered by the time we got to March or April 2021. Writing this summary was an adventure in past, present, and future tenses. I have changed or modified some of the text for clarity. I learned a lot; science is for people who like the steep part of a learning curve and Covid provided that. I knew about the innate immune system, but not as much as I do now. Readers will learn below what it is and how, perhaps, it can be managed to protect us in a future pandemic. I explain how important basic research is, how it gets done, and by whom. Pharmaceutical companies are also vital although some people dislike them, and a few companies have acted criminally to push opioids. They should not be lumped into one group. Manufacturing vaccines and drugs in large amounts is not simple. In the current case, most companies did a good job. I read the autobiography of Dr. Albert Bourla, the Pfizer CEO; he is an unusual fellow by any standards. The combination of basic and medical research done in universities, allied with nimble large and small companies has been immensely productive.
The summary below includes my own introduction to viruses. I taught at Columbia University’s Irving Medical Center where I had a research lab with talented students and post-doctoral fellows. For part of that time, I was the Associate Dean of Graduate
1
Students, involved with recruiting PhD and MD-PhD students to do research in our many laboratories. It was a pleasure to work with these young scientists and frankly, I miss them. I came to Columbia as a geneticist, but I taught cell biology and the structure of tissues and organelles to medical, dental, and graduate students. After a few years, I understood the subject (more or less), thanks to Mike Gershon, MD, who was the course director and is a superb teacher. Anne Gershon, MD is a pediatric virologist and cell biologist who helped bring us the chickenpox and shingles vaccine and has also been a friend over the years.
There are many people to thank, including Lakeville Journal editors Janet Manko and Cynthia Hochswender who want their readers to be scientifically literate. Marcie Setlow and David Scribner at the Berkshire Edge feel the same way. Norfolk Now, a newsletter in the town where we live, publishes the Body Scientific. Norfolk CT. has a rich scientific history and is the origin of the company that published the vital text, Molecular Biology of the Cell, as readers will see if they read to the end. The 7th edition just arrived. William
H. Welch, one of the 19th century physicians who modernized American medicine and helped found the Johns Hopkins Medical School, lived here. Dawn Whalen and Jen Pfaltz who run the Norfolk Hub for the Norfolk Foundation have been wonderfully helpful. For a scientist I am a bit of a technophobe, and they rush in to save the day.
Galene Kessin was The Director of Human Resources and Academic Affairs at the Columbia University Irving Medical Center. She ministered to thousands of driven scientists, physicians, and staff and has a complicated, not to say sardonic, view of scientists and physicians who fail in their administrative or management duties. I was one of them, but for the past 34 years she has tolerated me. Divine intervention, I think.
Scientific writing is constrained. There are few adjectives, no character development and (Heaven forbid!) no dialogue. Scientists write a lot, but the limitations got on my nerves. Besides, in science you can’t just make stuff up. That takes fiction, which is fun. The Famine of Men is a novel I wrote about a young virologist who has just become an Assistant Professor at a prestigious University in Boston (not Harvard). It’s her first lab and she is a little scared. The story is a lab bench view of how science is done. By informed chance she finds a virus that kills Leydig cells. These inauspicious cells live in the testes, where they make testosterone, which most men think is important. Women do not have Leydig cells and are unaffected by the virus. The Leydig virus, as our protagonist called it, is as infectious as Omicron or measles. Desperate attempts to create a vaccine fail. As males stop making sperm, lose their libidos and beards, and grow weaker, there are consequences—lots of them.
Richard Kessin Ph.D, is Emeritus Professor of Pathology and Cell Biology at the Columbia University Irving Medical Center. Reach me at Richard.Kessin@gmail.com. His website is RichardKessin.com. It contains a summary of science since WWII, and Body Scientific columns on many subjects. The subjects are skewed for rural readers and cover plagues of plants and people, vaccine resistance, GMO crops, PcB’s in the Housatonic River,
2
opioid addiction, and diseases of despair. There are columns on aging and its associated diseases, and on the virtues and limitations of the scientific method.
The columns have appeared on The Opinion Page of the Lakeville Journal and later in the Berkshire Edge and Norfolk Now.
Richard Kessin
Norfolk Conn.
November 2022
3
Beginning in Virology
We live in evolutionary competition with microbes—bacteria and viruses. There is no guarantee that we will be the survivors.
Joshua Lederberg (1925-2008).
A Founder of Molecular Biology, Nobel Prize Winner, Teacher
As an undergraduate I studied a virus called T4. That lab was my introduction to the power of viruses and molecular biology and working there remains a happy memory. The place was a refuge where I could do experiments that had never been done; it had interesting people and good scientists from all over the world, as did the neighboring labs. My boss and mentor, Chris Mathews, was 28, older than I was but not by much. He was already an Assistant Professor in 1966, but all these years later Chris and I have avoided senility or at least its worst effects. He reminded me recently that we published a good paper in the inaugural issue of The Journal of General Virology. Everyone should have such a mentor.
T4 virus has a surreal form: under the beam of an electron microscope, it looks like the first moon-lander, and it has a similar job: to land at a particular spot, in this case a protein protruding from the surface of a bacterial cell. This tiny machine has spindly legs and a spike that is essentially a syringe. Above the spike, where the lander’s crew capsule would be, a hollow body contains the virus’s DNA. The tube contracts to blast that DNA across the two cell walls and a lipid membrane and into a bacterial cell, the familiar E. coli. The DNA contains information that instructs the E. coli to make more copies of the virus.
Despite its austere name, T4 virus has a certain cachet in the world of molecular biologists because of all the information scientists have derived from it. What is the genetic material? How does it mutate? What are the physical properties of a gene? How do genes exchange segments? How do simple nanomachines like T4 turn on their genes in a particular order? How does T4 assemble the copied DNA into the capsule and then attach the tail? T4 and other viruses still provide tools to study fundamental problems in biology and medicine.
The wonderful thing about T4 for an undergraduate was that it works fast: experiments lasted a day, or more likely a night. When I added a few T4 viruses (or bacteriophages, as they are called) to a growing culture of E. coli cells and incubated the test tube at human body temperature (37 degrees centigrade), nothing seemed to happen for half an hour and then poof, the cloudy solution of bacteria disappeared, leaving a slightly
4
opalescent clear liquid. One or two viruses per bacterial cell had become 150 or more; and in an elegantly timed last act, the virus made an enzyme that dissolved the bacterial cell from within, liberating the new viruses to infect other bacteria. I was left with one milliliter in a glass tube. Chris noticed my astonishment and grinned. “Impressive, isn’t it? How many viruses are in there, do you think?” About 10 billion, as it turned out.

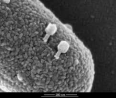


Bacteriophages were discovered by Felix d’Herelle in the 1920s. He and others thought they had therapeutic potential, but despite some success, the field did not develop in Western countries. Interest has revived. In the diagram, the virus has landed on a bacterium; the stem of the bacteriophage contracts and forces the DNA into the bacterial cell. From Ameneh Maghsoodi et al:
https://doi.org/10.1073/pnas.1909298116. In the lower panels viruses have been coated with a metal spray to block electrons and a scanning electron microscope beam has outlined their extraordinary shape. The last panel shows DNA released from the still visible phage particle.
All viruses are intracellular parasites and have the same modus operandi: bind to a specific protein on a cell surface, get their DNA, (or their RNA), inside, make more viruses using the equipment of the host cell, get out, and then infect a new cell. There are variations (and they matter), but a virus has no intent or malevolence; infection is mechanical.
Events get more complicated when a virus confronts immune systems or other defenses, as we will see with SARS-CoV-2. No invader, even a virus, attacks a cell without having the means to combat the host’s defenses, which are elaborate. They include an adaptive antibody producing system that takes time to activate but by astonishing means, remembers an invader. The innate immune system is always active and effective but has no memory. But in 1966, I was not concerned with the defense systems of bacteria or the immune systems of mammals. Much less was known about
5
immunology then and we took pride in simple focused experiments. Bacteriophages were the thing to work on. That has changed. Immunology and inflammation are now king, even for diehard bacteriophage partisans.
Viruses are small and because they pass through fine filters that retains bacteria, they were called filterable agents. Attempts to target viruses with drugs usually fail because they use the machinery of our own cells. Standard antibiotics, in 1966 the glory of medicine, do not work against viruses. One head of an infectious disease society declared antibiotics had defeated infectious disease, or to use one author’s phrase: turned the page on infectious disease. Hardly. Still, by the 1950’s and 1960’s science and medicine had bested polio, measles, rabies, mumps, rubella, whooping cough, diphtheria, and other virus and bacterial diseases with vaccines and antibiotics. Smallpox was eliminated in the late 1970’s. Tuberculosis, always a slow killer, could be treated from the early 1950’s. Since about 1995, new classes of antiviral drugs, the products of recent knowledge and spectacular advances in chemistry, have inhibited HIV and Hepatitis C viruses. DNA sequencing, molecular cloning, monoclonal antibodies, and other tools are now so routine that we sometimes forget how extraordinary they are, and at the same time, how much was accomplished without them.
Since the Body Scientific column began in The Lakeville Journal in 2010, there have been several viral pandemics, defined as vast infectious events covering continents. H1N1 influenza appeared in Mexico in 2009, H5N1 and several other flu viruses showed up after that. We rediscovered Ebola, Zika, and Chikungunya viruses in 2014 and 2015. The world is in its 7th cholera pandemic, although the disease is rare in the United States, reminding us that public health measures are the best defenses against disease. All the antibiotics in the world will be useless if drinking water is contaminated. Viruses and bacterial diseases will keep coming, whether new ones like SARS-Cov-2 or older ones like monkey pox virus and Zika virus.
Virologists, chastened by the 1918-1919 flu epidemic, thought another flu virus would drive the next big pandemic, but were slammed by SARS-CoV-2. Scientists and physicians were aware of coronaviruses because in 2003 the world had an epidemic of SARS, which infected 8000 people, killed 800, and then disappeared. Coronaviruses also infect camels and other animals (MERS or Middle Eastern Respiratory Syndrome) and the people who handle them, for whom it is exceptionally lethal, reaching 40%. Other coronaviruses cause mild colds and may provide some protection against SARS-CoV-2 if antibodies that cross react with SARS-CoV-2 are produced during these colds. What links different SARS viruses in a family is the similarity of their gene sequences and their crown-like appearance when viewed with an electron microscope, which can magnify 10,000-fold or more.
Scientists and physicians tend to be optimists and proud of their abilities and contributions, but that attitude can give the impression that all problems can be easily solved. With a new disease virus or other pathogen, or even a known one that has
6
mutated, this confidence is never a given. We have failed, so far, to make good vaccines for HIV, trypanosomes, malaria, amoeboid diseases, or Hantavirus, among others. We keep trying. New zoonotic pathogens, lurking in host animals, wait to infect humans or other animals. Skepticism is a scientific virtue and so is humility. The Body Scientific column has been preaching their value since 2011. We recommend genial skepticism, though. Yelling at people to get vaccinated does no good, although I confess to the occasional failure.
By historical standards the SARS-CoV-2 vaccines are a triumph; but I agree with a statement by President Biden’s former press secretary, Jen Psaki. When asked about who deserves credit for the vaccines and their distribution, she replied that with more than 600,000 dead Americans (now more than a million) and millions of victims throughout the world, no one should claim much credit. Still, in the summer of 2022, various investigators, including the World Health Organization estimated that the introduction of vaccines saved 20 million lives worldwide. That number will grow.
This story of Covid-19 began with columns I wrote from February 2020 to June 2022. In this narrative I have modified the columns because with new information coming at fire hose volume, leaving them intact was confusing. I have retained some of the order, which imposes a sense of timing and allows us to ask which of my assumptions, or those of other people, proved wrong. Errors and misconceptions are inevitable and essential in dissecting scientific problems. The same thinking applies to after-action reports in the military, case studies in medicine, and National Transportation Safety Board investigations. The mistakes I made in the columns I wrote since January 2020 are noted in brackets. Progress since the original columns were written appear in parentheses.
A Strange Pneumonia in Wuhan
Of the scourges the natural world can throw at us, a lethal new virus is one of the most frightening. At first, we don’t know where the virus came from, how many victims it will kill or leave debilitated, how to treat it, or how far and fast it will spread. Viral pandemics seem apocalyptic, and the response is often fear, or worse, panic. In March 2020, we were in the fear stage for Wuhan coronavirus (as it was then called), but we knew that science and industry would chip away at its biology and deploy to make vaccines and other treatments. (That has happened.) Technology and years of hard work have given us new weapons and tools, but public health measures and clear non technical communication are the most important tools at the beginning of pandemics. Our grades are not so good on that front.
7
Openness is the first rule of public health, even if the news is bad, otherwise no one has confidence in the public health authorities. The severe acute respiratory syndrome (SARS) infection of 2003 was kept secret for months by Chinese government authorities, giving the virus time to spread in China and then abroad. Eventually, quarantine and public health measures suppressed it, but not before 800 people died of about 8000 diagnosed patients (there were probably many more). The damage to trust between patients, governments, and scientists caused by such secrecy was severe and remains so. This reticence of authoritarians in government to confront bad news and change course has happened again with SARS-CoV-2.
Dr. Li Wenliang first noticed the “pneumonia of unknown origin” cases in 2019, as part of an informal surveillance system that he and other physicians had organized in and around Wuhan. When he reported these observations to his hospital colleagues, he was arrested and criticized by the police for spreading rumors and forced to sign a confession. Such are the dangers of science in authoritarian societies.
Once the problem was undeniable, Chinese scientists and physicians were aggressive in efforts to study, treat, and contain the virus, but as I learned from Bob Woodward’s book, Rage, CDC investigators and other scientists were kept out despite repeated requests by Dr. Robert Redfield, then the Director of our CDC to his counterpart in China, Dr. George Fu Gao. According to Lawrence Wright in the January 4, 2021, issue of the New Yorker (now a book), Dr. Gao was upset (Wright’s story says in tears), that he could not invite the colleague whom he had known for years. The health agencies of other countries faced similar problems. By this time, Chinese scientists were learning about a new and contagious virus was on the loose. In February 2021, a year later, a World Health Organization delegation made an inconclusive visit. The visit stirred more controversy, turning into an international issue. In July 2022, we still do not know the original reservoir of this virus, although the most recent work suggests the vicinity of Wuhan Live Animal Market.
Chinese scientists and physicians are probably not to blame for the breach in trust, but rather security officials and other bureaucrats marinating in the suspicions of an authoritarian regime. Dr. Li Wenliang, an ophthalmologist, died in February 2020 of Covid-19 contracted while he was performing eye surgery on an elderly woman. His obituary appears in the URL beside his photograph.
8
Dr. Li Wenliang first noticed the new respiratory syndrome and reported it to his colleagues.
Read his obituary at https://doi.org/10.1016/ S0140-
6736(20)30382-h2.


Dr. Shi Zhengli of the Wuhan Institute of Virology and her colleagues determined the sequences of the viral RNA genome from four patients with Covid-19. On January 10, she sent the sequences to an NIH repository for virus and other genetic sequences. It is not clear that she asked permission. That led to the Moderna, Pfizer, and other vaccines.
The treatments of the first 99 patients in Wuhan were described in the January 29, 2020, issue of The Lancet, a British medical journal. Half of the patients worked in a live animal food market. According to Chinese authorities, by February, the virus had spread to all Chinese provinces. On Feb. 4, 2020, there were 24,391 confirmed cases and 479 deaths, including Dr. Li. There was person-to-person transmission, through the air, which was frightening because such viruses are hard to contain. 2019nCoV (now SARS CoV-2) is not as communicable as measles, nor as lethal as Ebola, MERS, or the original SARS. It turned out to be bad enough. [It mutates more and faster than biologists and virologists, including me, thought it would.]
Of the eleven Wuhan patients who were initially admitted to hospital, a number were smokers or had compromised health. The Lancet paper described extensive efforts to help these patients, including mechanical ventilation and the use of experimental drugs. About half died. The remaining patients either recovered or were no longer critical at the end of January.
Left: Transmission electron microscopic image of an isolate from the first U.S.

case of COVID-19. The spherical viral particles contain cross-sections through the viral genome, seen as black dots. They are in the yellow band. This section is a thin slice through an infected lung cell that had been embedded in plastic.
Below: A free coronavirus is about 80 billionths of a meter in diameter. It is
hard to imagine something so small, let alone how dangerous it is. The
shape of cells is dynamic. Virus, in this case, exits from ruffles of the cell
membrane. From the CDC:
https://www.cdc.gov/media/subtopic/images.htm.
9


The United States had 11 known cases of Covid-19 as of Feb. 4, 2020—all people who had arrived recently from Wuhan and were isolated until they recovered. Local health authorities traced and talked to all contacts, providing food, thermometers, and other necessities. Whether those 11 cases or other sources would give rise to new ones was
the question at the time. [I was hopeful, based on the 2003 SARS cases, but the CDC was not. They were right].
There is a lot to learn during the first months of a new disease. An infection is not a sudden event like a gunshot wound. It is a gradual process, especially in the airways. Entering respiratory virus may be pushed up by cilia, millions of little waving oars that drive mucus and fluid upward in the airways. They are part of the innate immune system. Clearing the throat and swallowing kills viruses, which dissolve in stomach acid. Virus entry may be blocked by a coating of mucous on the cells of the bronchi or trachea; airways are lined with cells that secrete mucus. Sometimes the virus gets through these physical defenses and at that point, other systems of the immune system respond, as we will see. The host has many defenses against invaders, but the invading pathogen also brings weapons to stifle the defenses of the host. SARS-CoV-2 is particularly good at suppressing . In military terms, to paraphrase General Colin Powell, the enemy gets a vote.
My late colleague at the Lakeville Journal, Anthony Piel, a former counsel to the World Health Organization, pointed out in February 2020, that pandemics can be stifled if nations cooperate. Otherwise, there are too many types of viruses, at least 250 families, and they evolve quickly. The United States has always been a leader in Public Health and disease control and had a research program called Predict that searched for novel viruses before they jumped to humans. That program was stopped, at least temporarily. A pandemic response plan was shelved. The United States quit the World Health Organization and blocked a long-standing cooperative effort to let an American lab collaborate with the Wuhan Institute of Virology with NIH support. Because of earlier collaboration, American virologists knew what viruses the Chinese lab had discovered and sequenced. That is no longer possible. Anger is dangerous in a pandemic. People learn nothing when they are angry. For an extended report about of these early days
10
and the American response to it, see the remarkable first-hand account by Dr. Debora Birx, Silent Invasion, 2022).
Bats, Viruses, and Evolution
Caves shelter billions of bats, from Yunnan in China to Carlsbad in New Mexico. Bats are the only flying mammals; they fly out at night to feed on insects, fruit, or for vampire bats, blood. Their most extraordinary ability is echolocation; they listen in the dark and navigate by sonar, which allows them to find food, evade predators, and get back to their caves. They fly long distances, leave droppings widely and some of them bite. They are unique vectors of disease and being warm blooded, they are a good place to incubate zoonotic viruses. We think of rabies as a disease of the past, but in the Amazon forests many people die of rabies from bat bites every year. Many viral pathogens have been found in bats: Nypah virus, rabies virus, and coronaviruses, including SARS-1 and SAR-CoV-2, to name some. These viruses are often zoonotic, which means they can jump from animals to humans (and maybe back) through a bite, food contamination, or because people eat bats or other infected animals. Bat cells are remarkably like human cells. Bat lungs under a microscope are almost indistinguishable from human lungs.
In the winter, bats hang from the roof of caves while they hibernate or rest Their droppings accumulate as an ammonia-rich slush on the cave floor, which sounds revolting, but all that nutrient-rich guano harbors and feeds an extraordinary community of organisms, including strange predatory amoebae that my lab once studied (a story for another time). People harvesting guano for fertilizer are sometimes infected. Dr. Shi Zhengli and her colleagues at the Wuhan Institute of Virology sample these environments, bring the specimens back to their level 4 biosafety lab and determine the sequence of any viruses they can grow in petri dish cultures of human cells. It can be dangerous work. Dr. Shi’s laboratory is presently at the center of a conflict about how SARS-CoV-2 got loose on the world. Did they make the virus? Did SARS-C0V-2 virus escape the lab? Or was it a natural isolate that was ferried out of a cave by a guano harvester or unsuspecting scientist? I lean toward some version of the last two, but there is no way to be sure. [Two recent papers in Science suggest that the final evolution of SARS-CoV-2 did take place in or around the live animal market in Wuhan, from pieces of other viruses].
……..
The March 12, 2020, issue of Nature, an international scientific journal, has two dense papers on the discovery and sequence of SARS-CoV-2. Though some of the data were available on January 10, 2020, the narrative, assembled in one place, is gripping. The first article describes a 41-year-old man, straining to breathe, who was seen in The Central Hospital of Wuhan on Dec. 26, 2019. Four other cases reported in the second
11
paper were confirmatory; the patients were all infected by the same virus. The first victim had been sick for six days and reported fever, chest tightness, unproductive cough, pain, and weakness. Influenza, which might have explained the symptoms, was ruled out. He needed help breathing and had abnormal lungs seen on chest X rays and a CAT scan.
Twelve days after the appearance of symptoms, the patient landed in intensive care. His physicians put saline deep into one lung with a fine catheter and recovered 200 microliters of saline wash fluid—about four drops. They hoped to flush out a virus, and they did—about 100 million particles. Virologists and biologists are used to large numbers, but 100 million in 4 drops (0.2 milliliters) is a lot of viruses. Images of vast numbers of viruses budding from human cells are consistent. Unlike bacteriophage T4, SARS-CoV-2 infections keep producing until the host cell perishes by T-cell attack or apoptotic cell death, a form of cellular suicide that limits virus spread in mammalian or vertebrate hosts. The virus has genes and proteins that prevent this suicide.

This deformed lung cell has produced many thousands of SARS-CoV-2 viruses, shown as orange specks budding off the surface of the cell. The cell is deformed because it is probably undergoing apoptosis, a process by which a cell programs its own death. This scanning electron microscope image has been magnified thousands of times. The coloring has been added by computational techniques. Courtesy of the CDC Image Library.
RNA virus genomes are made of four nucleotide subunits: A, C, G, and U (rather than the similar T of DNA). In a particular order, they provide coded instructions for a cell to make proteins, just as a phonetic alphabet provides components to indicate sounds, syllables, and words. The genetic code requires three nucleotides to insert an amino acid into a growing protein–a phenomenon that is called ‘the triplet nature’ of the genetic code.
When virologists at The Wuhan Institute of Virology and another group in Shanghai sequenced several isolates of the virus, they found it contained almost 30,000 nucleotides. They learned they had a new coronavirus that was related to the SARS virus of 2003, to MERS, the coronavirus of camels, and to coronaviruses that cause colds. In extensive computer comparisons—a kind of 23 and Me for viruses—they learned the
12
new virus was also related to a bat coronavirus that they had found previously on expeditions to caves near Wuhan, but the new virus was not identical to that or any other known virus.

instructions for the famous Spike protein. ORF stands for Open Reading Frame, which means that the sequence has no interrupting mutations and has the information to make a protein. The box shows the length of the proteins in numbers of amino acids. Some of the sequences at the end of the virus genome may code for small proteins that inhibit a lung cell’s immune system. This is the gene structure of the original virus isolated and named in Wuhan: Wuhan-HU-1. The Number GenBank assigned it is: MN908947.
In Wuhan, scientists were concerned about the origins of the virus. They thought that the virus had made its way into a local indoor fish and seafood market where their patient and other infected people had worked. The market sold live hedgehogs, badgers, snakes, and doves, and the new coronavirus may have infected one of these species before it jumped to humans. Whether there a reservoir species or the evolution took place in the market is still unclear, but recent papers make the role of the live animal market has become more likely.
By the middle of January 2020, the novel pneumonia had spread, infecting more that 100,000 people in Wuhan; it had killed thousands. Hospitals were overwhelmed, despite the impressive efforts of the authorities to build new hospitals and an enforced stay-at home policy to break the chain of infection. At first there were not enough supplies, nurses, or physicians to treat all patients and a lockdown was instituted to slow the contagion. The United States, Italy, and other countries would soon be in this situation. At the time, many virologists and epidemiologists thought that in most places in the United States, a stringent lockdown would be impossible. They were right. (Even in China, in July 2022, stringent lockdowns continue to the great consternation of people in Shanghai and elsewhere). The effect of quarantine on an economy and people’s mental health is devastating.
Epidemics and the speed at which a disease spreads have been studied for a long time and mathematics has made its contribution with a factor called R0 (pronounced R naught). It describes the number of people a single patient infects, on average. With measles, R0 is very high, 12 to 18—think of the measles infection in Disneyland a few years ago. SARS-Cov-2 is less infectious than the measles virus, and its R0 is estimated to
13
be 2-3. (The mutations from the UK and South Africa variants add about 0.4 to that number, according to one report I read. One estimate for the delta variant with nearly 8. R0 for most influenza viruses is about 1.3. An R0 value above 1 means that an epidemic will expand; reducing R0 to 1 lets the infection smolder in the population. Reducing it to less than 1 drives the virus to extinction, as happened with the first SARS virus in 2003. Reducing R0 is the idea behind sheltering in place, hand washing, and personal protective gear, including masks.
Many of the viruses that afflict us use RNA, not DNA, for their genomes. Other than in viruses, this is rare. I do not know why some viruses use RNA, except that once the SARS-CoV-2 genome is in the cell, it can make new proteins and virus immediately, giving it a leg up on the immune system. The central concept of molecular biology is that DNA makes RNA; RNA makes proteins, and proteins can do almost anything, including making the bricks and mortar of a cell and providing thousands of chemical catalysts called enzymes.
Since the chemical structure of RNA differs a little from DNA, the virus brings two enzymes to perform tasks that animal cells cannot do. They are the Achilles heels of RNA viruses. One enzyme tacks the subunits of RNA together to make a genome copy (formally, an RNA-dependent RNA-polymerase). Many human viruses make a big protein containing sequences that need to be separated. Another unique enzyme is a protease that cuts proteins into smaller functional units, as many viruses do. Inhibitors that block the action of these proteases do not affect essential functions in human cells, but they stop the virus from making copies of itself. Inhibitors of similar enzymes in HIV virus and hepatitis C virus have controlled these diseases. Other drugs will appear (they have); it took more 10 years and a lot of excellent and relentless chemistry to produce the drugs that now control HIV and hepatitis virus.
In March 2020, reports from China and France suggested that a combination of hydroxychloroquine, an antimalarial drug and azithromycin, an antibiotic, stopped coronavirus reproduction. These reports described tests on small numbers of patients but on closer examination the experiments proved to be a muddle. Their lead author has been called before French scientific authorities to answer questions about the reliability of his work. (Dr. Didier Raoult, head of a microbiology service in Marseilles has been removed from his post, for this and other reasons). In larger clinical trials the drugs have turned out to be useless, either to control the infection or to block it from starting. Uninformed patients still demand it, and a few charlatans supply it.
14
Fear and Action
What the natural world can mount in the way of threats is greater than any virus we could build ourselves. A virologist would not have known how to create a delta variant of SARS-CoV-2, for example. The universe of viruses has ‘world enough and time’ to create new viral genomes by mutation or exchange between different viruses. Nature has the advantage of uncountable numbers of diverse genomes, time measured in years or even millennia, and selective pressure—if viruses do not change, they will be wiped out by immune systems in the animals they infect. When a new disease appears, we tend to blame humans, as if the natural world could not be so destructive without human help. Nature does not need our help.
The genome of SARS-CoV-2 is almost 30,000 nucleotides long, which is not huge by viral standards—T4 has 50,000 nucleotides, and monkeypox about 200,000. It had taken the scientists at the Wuhan Institute of Virology and universities in Shanghai, ten days to sequence and analyze the genomes of several isolates. The RNA sequence of SARS-CoV 2 was described in Nature in early March 2020, but the unpublished sequences had arrived at the NIH on January 9 or 10. That the Wuhan Institute of Virology director, Dr. Shi, deposited the sequence so fast is not the act of scientists hiding information. Perhaps the functionaries of the Chinese government knew nothing about sequencing or GenBank. My guess is the critical sequence information whizzed by them.
From that sequence, skilled virologists can make vaccines and begin other studies. Dr. Barney S. Graham is an expert on how to make a virus provoke the human immune system. He had been working on RNA viruses and had created a vaccine against Respiratory Syncytial Virus, which causes a serious and common pulmonary disease in children. (This vaccine recently passed its clinical trials). His department quickly began to study SARS-CoV-2. One of the research fellows at NIAID, Dr. Kizzmekia Corbett, did much of the first analysis, where experience counts. Having done the basic work on SARS-CoV-2, at the National Institute of Allergy and Infectious Diseases, NIAID licensed the project to Moderna, a manufacturing company with expertise in RNA vaccines.
15

Barney Graham, MD, PhD and Kizzmekia S. Corbett, PhD worked at the National Institute for Allergy and Infectious Diseases. Their lab has worked on vaccine and monoclonal antibody development for SARS-CoV-2, Respiratory syncytial virus, influenza, Nypah, Zika, HIV, Ebola, and other emerging pathogens. Dr. Graham recently retired. Dr. Corbett was a research fellow and designed the genetic element used to produce the Moderna vaccine. She is now an Assistant Professor at T.H. Chan School of Public Health at Harvard Medical School.
Between April 20, 2020, and the widespread availability of vaccines, the best we could do, beyond testing, isolation, and supportive measures, was to find drugs that slow the virus infection until our immune systems can mount a directed offence. We would be wise to find better ways to protect front-line nursing and medical staff. We should wear masks ourselves (see below). There will probably be a new surge of virus in the fall of 2020 (there was) and it would be unfair to ask nurses, doctors, and other medical staff to work in emergency rooms and intensive care units without better protection than they have had.
Several vaccine candidates entered phase 1 clinical trials in the late spring and early summer of 2020. They will be tested for safety, dose, and the immune responses they provoke. The vaccines usually present humans with the coronavirus Spike protein whose role is to bind to a protein that protrudes from the surface membrane of human cells. Starting in February 2020, it will take at least a year to complete Phases 2 and 3. There will be intense pressure to speed the process up. (Recall that there was.)
Drugs that slow viruses like SARS-CoV-2 are also entering clinical trials. Remdesiver blocks the production of the RNA genomes for new viruses. More trials are necessary according to Dr. Anthony Fauci, for whom this is familiar territory from the battle against HIV. Tests of dosage and early use in the course of an infection may make remdesivir more effective, but there were mixed results at the beginning. We now have Paxlovid and other drugs, described below. A drug or vaccine does not have to be completely effective; it needs to tip the balance in the patient’s favor.
Prof. Arturo Casadevall of The Johns Hopkins Bloomberg School of Public Health speaks of layered defenses. What he has in mind is the convalescent antisera of people who have recovered from Covid-19. This approach to stopping the virus by supplying antibodies to the circulation has entered clinical trials in the United Kingdom and will soon be in double-blind trials in the United States (it is). Anecdotal evidence (a scientific oxymoron) suggests that Italian patients benefitted from convalescent serum. What seems to be happening is that post-immune serum and particularly combinations of monoclonal antibodies mitigate the disease, if given early in the infection (January 2021). SARS-CoV-2 virus makes a huge number of copies of itself, and the delta variant (not to mention Omicron) makes more. It may be essential to intervene when there are fewer viruses, or less damage has been done from inflammation. Inflammation is a
16
general defense, but the cells that cause it: neutrophils, eosinophils, and others are destructive and release enzymes and toxins that can cause serious tissue damage.
Spread of SARS-CoV-2 in the United States
In February and March 2020, there was increasing community spread of SARS-CoV-2 virus in the United States. Community spread means that the infection cannot be traced to a single source and that the virus is loose in the population. The first American fatalities came from a nursing home in Washington State, but soon the epidemic no longer had a single focal source. In March 2020, the increase in infected people seemed to be exponential and track earlier events in Italy, which was in a crisis with 14,000 cases, 1000 dead, and the country shut down. The US epidemic is (was) at an earlier stage with more than 1629 cases and 41 dead according to the CDC.
It is not enough to count sick people. Many people have subclinical infections but are still capable of infecting others. They drive the spread of the disease, especially in the absence of good tests for the virus. Why such people are not seriously affected is a conundrum, or if you are an optimist, a clue. The human population is diverse, and some may have primed immune systems that protect them. An answer will come, and it will be critical to stopping this and perhaps future epidemics. Even if we can cut the production time of vaccines in half, to six months, to depend on vaccines for every outbreak of a new and dangerous virus would result in serious trauma to society. Perhaps there are ways to make a disease less severe in early days, as we will see when we come to the innate immune system and new antiviral drugs.
In the meantime, large swaths of the seemingly healthy population, especially in hard hit areas, must be tested for coronavirus to determine how many silent infections there are. Testing distinguishes coronavirus from other common infections and reduces hospital visits. It tells us the state of the epidemic on a local basis, especially when wastewater is tested. Molecular testing also picks up the effects of hand washing and social distancing, and when drugs or vaccines become available their effects can also be studied without waiting for symptoms.
In the early days of the pandemic, we were monumentally bad at delivering test results. It was not for want of scientific skill, but rather regulatory and other hurdles intrinsic to our decentralized medical system and democratic society. Depletion in government agencies that normally prepare for such disasters also had a negative effect. CDC made an error in preparing test kits: one of the reagents was contaminated by fragments of viral genome, which made the test useless. No other tests were approved and the one that was had to be sent to CDC for processing, which was a time-wasting process. WHO had offered a working test, but CDC declined to use it, according to some reporting. The CDC is a discovery, diagnostic, and detection focused agency; they are not equipped for
17
large-scale manufacturing of a test or a vaccine. These are an under-appreciated skills of their own. Pharmaceutical companies have the facilities and expertise for this task. Mistakes and malfunctions, scientific, administrative, and political, will be sorted out in what I expect to be critical after-action reports. One has been commissioned by the CDC Director, Dr. Rachel Wilensky and is underway, at least for the CDC.
For the very sick, the task was to find hospital beds and medical staff. Physicians and nurses need ventilators and oxygen to keep people breathing when their lungs are severely affected. Fatalities increase when hospitals are overwhelmed, and the supportive measures of modern nursing and medicine cannot be brought to bear. Exhausted nurses, physicians and staff are a recurring theme in this tragedy. There is not enough medical reserve in this country to deal with a pandemic such as SARS-CoV-2. The Public Health Service has about 3500 nurses and doctors to deploy, and that is not enough.
Masks, Mistakes, and Progress
In March and April of 2020 people were arguing about masks and disease prevention. Virologists and others initially thought that because the Covid-19 virus is so small, it would pass through a mask. We were wrong, fortunately. [I should have been more cautious.] Viruses also come in lipid droplets, which, from the point of view of the virus, may be adaptive, because droplets (more graphically, think gobs) deliver vast numbers of viruses. One paper I read said that it takes about 1000 virus particles to initiate a SARS-CoV-2 infection, but that seems arbitrary. A droplet 1 micron diameter would fit a lot more than 1000 viruses. Masks block droplets, if not single viruses. The technology of masks can be improved, although N95 masks are effective. (The NIH has recently issued a request for proposals (2022) to produce better and more comfortable masks; there are already many candidates).
When people inhale droplets of mucus containing SARS-CoV-2 corona viruses, the viruses populate the upper respiratory tract and then infect cells more deeply into the lungs. If they survive the clearing power and barriers of the airways, the viruses enter human cells and replicate in the throat and lungs and set off a strong innate immune response and then an adaptive, antibody based immune response, both described below. (Vaccines that stimulate immune responses in the upper respiratory tract’s mucosal cells are under development for many viruses.)
18
A review on airborne transmission by Drs. Kimberly Prather, Chia C. Wang, and Robert T. Schooley was published in the journal Science. They distinguish large infectious particles and small ones—both emerge from a cough or just breathing by asymptomatic individuals. The largest droplets, a tenth of a millimeter in diameter could contain millions of viruses but sink within the now famous, but arbitrary, six feet. These respiratory droplets contaminate surfaces where virus particles may remain infectious. These data are a bit fragmentary, but they are helpful.

A cough and a strobe light. A lot comes out— in two forms. The larger blobs of lipid can contain thousands of viruses. The lighter particles float in the air as aerosols. When inhaled, their many viruses can breach the body’s defenses. From the Science paper quoted below.
The larger particles are about 1 micrometer in diameter and could contain thousands of viruses, each with a diameter measured in nanometers, or 1/1000th of a micrometer. Aerosol vesicles are smaller, accumulate in room air, and are too light to sink rapidly. Aerosols have a long history in microbiology—Louis Pasteur saw them on beams of light in dark rooms and knew in 1864 they were a source of contamination, which he announced at a tumultuous meeting at the Sorbonne. Viruses as we now know them were not identified until the 1890’s, although the word virus existed to connote something morbid. One phrase used in prior centuries was the charming but not very precise, ‘morbitudinous matter’.
Once a particle containing viruses enters cells in the lung or infects cells in the sinuses and throat, new viruses can be made almost immediately because the virus contains messenger RNA that is translated into new virus. Think of a thousand virus particles attacking a small area of an alveolus, a viral Shock and Awe. Our immune systems do not have much time to repel the attack. Remember the patient in Wuhan who had hundreds of millions of viruses extracted from a site deep in his lung. (Perhaps I missed it, but the paper did not say whether the patient survived).
Our defenses before and during an epidemic are largely limited to public health measures until there is a vaccine, drugs, or other preventative treatment. For the
19
scientific paper behind these thoughts, paste: DOI 10.1126/SCIENCE.ABC6197 into any search engine. The information is readable and free to download. It is part of a movement for free access to scientific papers. DOI stands for Digital Object Indicator— not poetic perhaps, but it gets you to the evidence.
The Structure of Clinical Trials
All vaccines, drug treatments, and therapies pass through clinical trials, which have rules derived from painful experience that include cheating by investigators, using patients who have not consented or who are not capable of consent, and conflict of interest on the part of the investigators. The idea is to protect volunteers and patients and to do no harm, as well as getting a reliable idea about effectiveness of a vaccine or drug. Getting permission to start a human clinical trial includes an analysis of the likelihood of success, the pre-trial evidence, and statistical requirements. Phase III trials are a major commitment of time and resources.
The groups doing clinical trials must register them with an organization at the National Library of Medicine at the NIH. Anyone can find the list of clinical trials for a disease or condition at www.ClinicalTrials.gov. If you are interested in joining a SARS-Cov-2 clinical trial (or any clinical trial), you will also find medical centers involved in the trials at that
website (enter code identifier NCT04470427 for the Moderna vaccine). Clinicaltrials.gov lists clinical trials for all diseases, drugs, devices, and conditions, with contact information. There are many thousands, but there is a good search function.
Trials have three stages. The first, which uses only a few volunteers, makes sure a vaccine or drug causes no harm and establishes a safe dose. The second phase engages more volunteers, hundreds perhaps, and looks for adverse reactions and the activation of the immune system (in the case of vaccines), but does not yet concentrate on efficacy, although with hundreds of people, positive or negative effects may be found. The third phase tests protection from infection and requires thousands of volunteers, male and female of all ages and ethnicities to get statistically significant answers. The number was usually 30,000 in the Covid-19 vaccine tests. Neither physicians nor patients know whether an injection contains vaccine or placebo; hence the trials are called double-blind. Well-designed clinical trials are the most critical part of solving Covid-19 or any other problem. They are expensive and may fail—the FDA keeps a humbling list on its website of vaccines that looked to be excellent through phases I and II, but which failed in Phase III. The Merck SARS-CoV-2 vaccine was one.
The British have made progress. They have the advantage of the National Health Service and its hundreds of hospitals (one of which saved Boris Johnson, who seemed grateful). The NHS uses one clinical trial protocol and a unified reporting system for more than a hundred hospitals that are equipped and trained to do this work. It can move fast. The
20
system is called RECOVERY (Randomized Evaluation of COVID-19 Therapy) and has already yielded results.
One RECOVERY study proved the value of dexamethasone, an anti-inflammatory steroid drug used for Covid-19 patients to control inflammation. Other data showed that hydroxychloroquine is useless. Several drugs that are useful against HIV and might have worked against SARS-CoV-2, even should have worked, did not help. According to Science reporter Kai Kupferschmidt, these three results changed the standard treatment of Covid-19 over a few weeks.
Monoclonal antibodies that bind to the SARS-CoV-2 virus and neutralize it are being tested for treatment and prevention. Former President Trump believed they cured him and perhaps they did, but proof awaits clinical trial completion (now done and effective for acute infection with the then existing coronavirus variants). A January 2021 study from Regeneron, a pharmaceutical company, concluded that they are useful early in the infection during the period before a patient makes his or her own antibodies, but not after. Their efficacy varies with the Covid-19 variant causing the infection. (Omicron and its variants appeared in vaccines and as monoclonal antibodies in September 2022).
One of the stranger stories I came across while reading this literature involved antibodies from llamas, alpacas, and camels. Antibodies from these species are one tenth the size of human antibodies. No one knows why. But it is possible to produce monoclonal versions that bind to the Spike (or any viral protein) of coronavirus with extraordinary tenacity. The hope is that the small antibodies will block virus entry into lung or other cells. Camel and alpaca antibodies are unusually tough, and the authors of the paper are testing them by inhalation against SARS-CoV-2 in animal experiments.
Why are mRNA Vaccines Different from All Other Vaccines?
Some people, confronted with the SARS-CoV-2 vaccine, declined it because they thought it was developed in a rush. The question is not whether the Moderna, Pfizer or other vaccines were developed too quickly, but rather why traditional vaccines took so long to make. The classical vaccines were made in the days before DNA or RNA genomes could be sequenced and before viruses could be quickly compared at a detailed molecular level to find what had changed in the preparation of the vaccine.
Polio, measles, and mumps vaccines were created in the 1950’s and 1960’s. They are all RNA viruses, as is SARS-CoV-2. At the time, there was no way to determine their RNA sequence because sequencing methods were not developed until the late 1970s. These and other vaccines were triumphs, but we did not know the genes that coded for essential functions of the virus or how they were changed in a bacterium or virus used
21
to make a vaccine. Virologists could see the shape of viruses in electron microscope images (viruses are too small to see in light microscopes), but vaccines took years to make.
To make a vaccine, scientists had to inactivate or weaken the virus, or bacterium. Inactivation with formaldehyde killed the virus and sometimes this inactive structure works as a vaccine, but often live viruses provoke the immune system better than a virus or bacterium killed with formaldehyde. Thus, the Salk polio vaccine contained dead virus and the Sabin vaccine contained a weakened but live virus. We did not know how the RNA sequences were changed in the Sabin vaccine virus. My Columbia colleague, Vincent Racaniello and his collaborators were the first to sequence the polio virus genome. There were only a few changes out of the 6000 ribonucleotides that make up the Sabin polio vaccine virus. This was a shock. It can and does revert to a disease-causing strain, but rarely. Using knowledge of the sequence, a new live virus vaccine has been made that has more changes and does not revert.
The classical vaccines were created by growing the viruses in cells in petri dishes or in animals, recovering newly made viruses, diluting them dramatically, and then growing them again and again. This process is called passaging the virus and eventually a mutated virus emerges that can activate an immune system without sickening the host. Finding such a mutant virus that could activate the immune system without causing disease often took years. The story of the development of the polio vaccines has been ably presented by New York University historian of Medical Humanities David Oshinsky in his book Polio: An American Story. Each defeated virus or bacterium has its own riveting narrative and Dr. Oshinsky’s on the polio virus and the people who developed the vaccines is particularly good.
The first anti-viral vaccine, against rabies (also an RNA virus), was a daring venture into the unknown. In 1885, desperation and an insistent mother whose son had been badly bitten by a rabid wolf, played a role and fortunately, the vaccine worked. Or at least the boy recovered. Rabies virus migrates up neurons to the brain and that takes time. The vaccine, if given soon enough after a bite by a rabid animal, seems to prevent disease. Louis Pasteur and his colleagues did not know about viruses, but they were effective scientists and knew how to use controls with experimental animals, which they could not do when they treated humans. Rabies was (and is) such a horrifying disease that the apparent success of Pasteur’s experiments, widely reported, changed the public’s perception of medicine and its utility.
SARS-CoV-2 vaccine candidates based on sequencing information entered phase 1 clinical trials in the late spring and early summer of 2020. They were tested for safety, dose, and the immune responses they provoke. Vaccines usually present humans with the coronavirus Spike protein whose role is to bind to a protein that protrudes from human cells. Starting in February 2020, scientists knew it would take at least a year to complete Phases 2 and 3. There will be intense pressure to speed the process up. That
22
involves risks, but they may be inevitable. (The timing and pressure turned out to be about as predicted).
At the end of July 2020, the data from phase 1 and 2 trials of three vaccine candidates were released—one by Moderna, one by Pfizer, and the other by the Oxford/AstraZeneca vaccine team, which used a different technology. All vaccines provoked a robust immune response in healthy volunteers and passed their clinical trials.
The vaccines employ different strategies to provoke the human immune response and entered large phase 3 trials to determine efficacy. Two have been approved for emergency use in the US, the UK, and other countries. The Oxford/AstraZeneca vaccine is being administered in the UK and other countries and is available in the United States (it ran into difficulties but is still one of the most used vaccines). The Johnson and Johnson vaccine began distribution on March 2, 2021. There are many other candidates, but the important part of this process is not only the creation of the vaccine, but the size and excellence of the clinical trials, including the power of their statistical analysis.
‘Waiting is the Hardest Part’
On October 25, 2020, we were waiting for medical centers that administered Moderna vaccine or placebo in Atlanta, Houston, or other hotspots of infection to report on the numbers of people in their trials had Covid-19. From my inquiries at the NIH, the Moderna vaccine was the only one in a Phase 3 trial that was fully subscribed by October 25, 2020—30,000 people had volunteered and have had both shots. The similar Pfizer vaccine was a little behind. Other vaccines, from Oxford/AstraZeneca, Novavax, and Johnson and Johnson were all around the same stage in October 2020. (All but Novavax were granted Emergency Use Authorization. The Novavax vaccine was approved in the summer of 2022). It is based on production of native Spike proteins in insect cells growing in a culture medium, but the vaccine itself carries no genetic material, only protein.
Before starting their Phase III trial, Moderna and all other companies, with the cooperation of FDA scientists and statisticians, had decided on how many patients with Covid-19 had to be reported before the books on the double-blind trial were opened. At that moment, investigators would learn which volunteers had received the placebo, and which has received the Spike coding mRNA.
23
In the best of worlds, the sick patients would have received placebo and all the people who received vaccine would be healthy. If both groups had an equal burden of disease, the vaccine fails. If the people who got vaccine had half the cases of the people who got placebo, that is defined as a success. For scientists and physicians involved with the development of these vaccines, opening the register of cases is a nerve-wracking moment.
We need to learn about each sick patient in the trial. How long did they have symptoms? Did they need oxygen or a ventilator? Did anyone die? What was the viral load in each patient? Was the patient making anti-viral antibodies and T-cells? Are there side effects? Do tests in Atlanta, Toronto, and Phoenix report statistically comparable results? A lot of information can be teased out of a well-designed trial, including fraud in reporting.
The Pfizer vaccine data from 14,580 placebo patients and 14,550 vaccinated patients, was as follows: Four months after vaccination, 185 volunteers who had received placebo were ill with Covid-19 and 30 of them were severely sick. Eleven of the vaccinated patients had mild disease; there were no cases of severe illness. The vaccine efficiency was 94.1% or more realistically between 89.3% and 96.87%, given the limited numbers involved.
| Placebo | 14580 volunteers | 185 with Covid | 30 severely sick |
| Vaccinated | 14550 volunteers | 11 with mild Covid | None severely sick |
Pfizer and Moderna had been making vaccine during these trials so as not to waste time. To see the Pfizer vaccine data from the New England Journal of Medicine, see: DOI: 10.1056/NEJMoa2035389. The author put a lot of information on a single page. The summary also warned people about what we did not know. The most important area of ignorance was that no one knew how long resistance would last. Resistance arose after months, but after two injections and two booster shots, even if people got sick, they recovered. These infections could be due to the failure of immune memory, the evolution of the virus, or both. The sustainable resistance to severe disease is probably due to T cells, which kill SARS-CoV-2 infected cells. were se and provided 94% efficacy
Moderna and Pfizer prepared applications for Emergency Use Authorizations. A standing committee of the FDA with independent reviewers studied the data and in mid December they voted and gave preliminary authorizations. In February 2021, all had received an Emergency Use Authorization by the FDA.
……..
The anxiety of waiting for vaccine results has a history that is worth a short digression. Louis Pasteur and his students made the first designed vaccine in 1879, for anthrax infection of sheep. Pasteur was a controversial figure and provoked a lot of challenges,
24
which he usually won. One of these led to a clinical trial at a farm in Pouilly-le-fort, a village to the southeast of Paris. Dr. Patrice Debré, a biographer of Pasteur and himself an immunologist, called it The Wager of Pouilly-le-fort. Twenty-five sheep were vaccinated with a weakened anthrax strain and 25 were not. After two weeks, the vaccinated sheep got a boost of vaccine (a lot like the Moderna and Pfizer coronavirus vaccination schedule). Two weeks after that, all fifty sheep were given a lethal dose of Bacillus anthracis. (Debré’s biography of Louis Pasteur has been translated into English and has an extensive account of the anthrax vaccine experiments).
Pasteur did not come to Pouilly-le-fort to inoculate the sheep with lethal Bacillus anthracis; that was done by Emile Roux and Charles Chamberland, two of his most effective assistants. Overcome with anxiety, Pasteur paced in his laboratory at the École Normale Supérieur in Paris, while Chamberland and Roux carried out the injections of lethal anthrax and then came back to Paris. According to Professor Debré’s account, a large crowd gathered for the outcome; it included reporters, scientists, and heads of agricultural societies as well as many farmers. People knew the importance of the outcome and Louis Pasteur was famous for solving other agricultural and industrial problems, (he had not yet moved on to people) so there was high hope. Success would change medicine and agriculture; failure would set back vaccines and medicine for decades. Two days after injecting virulent anthrax, nobody from the Pasteur team was at the farm in Pouilly-le-fort, and it was left to a veterinarian, one Dr. Rossignol, who had organized the event, to send a telegram to Pasteur. “Succès épatante! (Stunning success), it said. Twenty-five sheep were dead or dying; 25 vaccinated sheep in the same pasture were healthy.
25
Pasteur and his colleagues went on to make vaccines to control chicken cholera and rabies. The rabies vaccine was the first used on humans and convinced the public that vaccines and science could transform medicine. I cannot do that story justice here, but there is a film, The Life of Louis Pasteur, starring Paul Muni, which does tell his story. The film won an Academy Award for best picture in 1936 and is available on Netflix. It compresses the story, but for a Hollywood rendition it gets the facts about right. It is, to be sure, a little adulatory, as are most accounts of Pasteur’s life.
……
The placebo arm of the Pfizer, Moderna, or any other trial becomes ethically untenable when the results are clear. Placebo treated patients must be notified and offered real vaccine. A friend who was in this trial was notified that she had received placebo and got the vaccine in early January 2021. All treated patients, in the case of the Moderna and Pfizer vaccines (and others), will be followed for two years to learn how long antibody and T cell responses last and to look for late side effects. Those results, properly studied, could lead to licensing of the vaccine. (It has been licensed). In the meantime, vaccines are administered under an EUA or Emergency Use Authorization.
In January 2021 there was enough FDA approved vaccine to distribute widely. Some vaccines need to be frozen on dry ice, but Fed-Ex, UPS and other companies are prepared for frozen packages. Scientists and clinical labs know how to handle cold temperature—many of their supplies arrive on dry ice. Cold temperatures will not be the rate-limiting step. The Johnson and Johnson vaccines should be ready shortly (they were), as will the Novavax vaccine (delayed until 2022). Distribution will be through established channels. I do not believe the military will be heavily used, except to vaccinate their own people and dependents (no small task) and perhaps for distribution in difficult places. [National Guard and Regular Army troops have effectively assisted the vaccine rollout. They provided order, calm, and confidence, as a physician friend who got her vaccine at the Javits Center in New York City told me. Kudos to them.]

The worries about distribution, access, and injection are real, but the United States has done this before. In 1947 a smallpox outbreak hit New York City. Within a week, millions of people had been vaccinated, an effort that remains a seminal moment in the history of public health.
26
The Adaptive Immune System Makes Antibodies and T-cells that are Specific for Different Viruses or Bacteria
Oh God, how I loved this new science of microbiology done in the open air!
Dr. Emile Roux
The first scientists to make a vaccine from scratch were led by Louis Pasteur, as we have seen. Pasteur had made the discovery years before that fermentation is carried out by minute organisms, including bacteria and yeast, and without them wine does not ferment, bread does not rise, meat does not rot, and infections do not occur. There was extraordinary, even furious objection to the germ theory of fermentation and disease, especially from chemists in Germany, but Pasteur was right. Emile Duclaux, one of his students, later the first head of the Pasteur Institute, called the germ theory fertile: it gave rise to microbiology and immunology, vaccines, surgery without infection, and safer childbirth. Eventually, it eliminated infections caused by contaminated milk or water, led to better wine, beer, and cheese, and created industrial advances too numerous to list. Over time, child mortality from infectious diseases plummeted. Even now, fertile is not a word normally associated with a theory, but it should be. Fertile theories help people think.
The smallpox vaccine, in 1799, was first, but it was an outlier, preceding others by about 80 years. Why the delay? It took that long to create the idea and substance of microbiology and the germ theory of disease. Once Louis Pasteur, Robert Koch, Joseph Lister, and others knew that a bacterium caused anthrax, Pasteur and his students managed to weaken Bacillus anthracis and that gave rise to the first vaccine against animal diseases, as we have seen. The opposition continued to be furious, but Pasteur knew the power of his ideas and he was a formidable debater and showman. He reminded his opponents that Fortune Favors the Prepared Mind. Pasteur inspired allies like the great surgeon Joseph Lister, who introduced sterile techniques into surgery after reading Pasteur’s papers. The opposition retreated, but it took decades.
Fortune also favors the prepared immune system, about which Pasteur knew nothing, except that animals and people became resistant to reinfection. He knew that when people recover from an infection, they are usually immune and can then safely nurse the sick. He knew about cowpox and the immunity it provided to smallpox. Nonetheless, deciding to make new vaccines was a leap. It provoked an anti-vaccine response, which continues.
27
The press responded to smallpox (1803) and rabies vaccines (1885). Opposition to vaccination is not new.
There was another success from the Pasteur Institute in 1894. It was led by Emile Roux, who had been instrumental in creating the earlier vaccine. It was a serum against diphtheria, then the most feared disease of children. It was made from horse antibodies and managed to reduce the mortality rate of children in Paris hospitals by 50%. The German scientist Emile von Bering isolated the diphtheria toxin and inactivated it, which gave rise to a vaccine. The response of the public was positive. In France, Roux was lionized.
Two images of the response to diphtheria treatment. Antisera work to stop the infection, but with more difficulties than a vaccine which was an inactivated toxin.
…….
Let’s look forward about 140 years and ask how proteins are made and how immunity occurs. Most of the Covid-19 vaccines are designed to present a SARS-CoV-2 Spike protein to the human immune system and provoke the production of circulating
28
antibodies that bind to the virus, or killer T-cells that recognize infected cells and punch holes in them.
The Spike protein is a long string of amino acids, small molecules that snap together like Lego pieces. The acid group of one reacts with an amino group of the next to establish a chain that grows by addition. The process is called Protein Synthesis or Translation (of an RNA strand into a protein chain). You-tube provides many animations. The first amino acid in a chain is always methionine; the second could be any of twenty. By the time we get to three amino acids there are 400 possibilities, then 8000 (400×20) and so on. A protein may have hundreds or even thousands of amino acids in its chain.
Each of the twenty amino acids has additional different groups of atoms that create shapes, surfaces, helices, and other structures in a finished, folded protein. The number of possible protein shapes is astronomical, including some, that are familiar objects that look like water wheels or a propeller. The combinatorial property of the genetic code and the shapes in can produce in proteins resembles that of a phonetic alphabet, 26 letters which can code for all of literature.
The Spike protein, on which most of our vaccines depend, has about 1200 amino acids. Evolution took advantage of random mutation and the diversity it provides to select an order of amino acids that folds into a Spike shape. Spike proteins bind tenaciously to ACE2, a protein that is part of a system that regulates blood pressure in lung cells and blood vessels. (The blood vessels are attacked by SARS-CoV-2, causing clots, strokes, and heart attacks. For this reason, anti-coagulation drugs are part of therapy for Covid-19.)
The Spike protein is still changing—genetic changes occur spontaneously (especially during long Covid) and can lead to a Spike protein that binds ACE2 more tightly or has other ways to make the virus more potent. That is what appears to have happened with the UK, Brazilian, and South African and Indian (delta) variants of the coronavirus. It is classic evolutionary biology—huge diversity in an immense population of viruses, followed by winnowing natural selection of a few variants that grow quickly and avoid host defenses.
After a vaccination or illness, the immune response subsides, but antibody-producing B cells and cell-killing T cells are banked to provide a memory of past infections. When infection with a previously encountered virus occurs, thousands or millions of banked lymphocytes start to divide and quickly produce enough antibody or killer T-cells to block or minimize the infection. These are called memory B and T cells. With some vaccines the banked cells last a long time (measles, yellow fever, smallpox, mumps, and rubella), but with others, responsiveness lasts a few months or years (whooping cough, tetanus, influenza). Your deposits of memory B cell and T cells are the most important bank accounts you own.
29
A healthy human being facing a novel virus is at a disadvantage because it takes time, perhaps two weeks, to produce to produce antibodies and killer T cells by cell division expansion from single cells. Most B-lymphocytes in the blood, spleen, or bone marrow
are dormant, their genes are shut down, their DNA folded up and inactive. Under a pathologist’s microscope, the lymphocytes form a sea of blue cells. Each lymphocyte has a different antibody protruding from its surface—one lymphocyte cell, one antibody. Billions of different lymphocytes, each waiting for something (an antigen) to bind.
Suppose we vaccinate the owner of these dormant B-lymphocytes and T-cells with Spike protein. What happens? Among billions of lymphocytes, a few recognize the shape of a Spike protein fragment. The fragments have been predigested (a process that is beyond
us for the moment). A signal goes to the dormant nucleus, notifying the cell to unwrap its DNA and start to divide. For purposes of illustration let us imagine that they divide twice a day. In two weeks, one B or T cell, will, in theory, be 213 B or T cells (more then 16,000) with the same antibody on their surface. At some point the antibody is released into the circulation. This process is called clonal expansion and is the basis of immunology. During clonal expansion of B cells, more mutation of antibody coding genes takes place which leads to an even tighter affinity for coronavirus.
There is a lot else going on during antibody production. We cannot have antibodies or T cells reacting to our own proteins or we will suffer from autoimmune diseases. Such self-reactive lineages are killed off—B cells that react with the host are killed in the bone marrow while reactive T cells are killed in the thymus. As the B and T cells mature, rearrangements of DNA take place and regions of the gene are mutated to create even greater antibody diversity. As B-cells mature, they find their way to lymph nodes or other immune organs like the spleen. A second booster shot, as in the case of anthrax at Pouilly-le-fort or the current coronavirus variants, increases the number of cells and antibodies by perhaps 10-15-fold and increases their affinity for virus. Subsequent boosters do more.
It takes a lot to become a B cell or T cell. Most of all it takes huge numbers and a great diversity of antibodies. B and T-cells do not divide without help from other cells that secrete proteins that stimulate them to divide, but two weeks after injection of Spike protein, a vaccinated person will have lots of antibody and many T-cells. If the infection has not already caused terrible damage, it will probably be controlled.
Early in Infection, the Innate Immune System is Our Best Defense
In the middle of an explanation of clonal expansion of lymphocytes, a woman in the second row of my class, (I was just starting as a teacher) asked, as politely as she could, “Dr. Kessin, are you sure? This sounds like baloney to me.” I was smart enough to smile. She had a point, after all. I explain that immunology is confounding because it breaks so
30
many conventions of biology, that it is hard to believe. How is it possible that the immune system can recognize millions of chemicals, and not recognize a person’s own molecules? How does it create diversity in its antibodies? There is a lot of DNA in a human cell nucleus, but not enough to code for a million different antibodies. How does it avoid creating autoimmune diseases? How does it sequester memory cells? How does it deal with novel infections if it takes two weeks to activate the adaptive immune system? I am not sure I convinced her.
The idea that tiny bacteria could kill was also hard to believe in the 19th century. It was easier to believe that the little rods found in the blood of anthrax infected animals were the product of a disease rather than its cause. Immunity as a problem has taken more than two hundred and twenty-five years to work out, starting with Jenner’s smallpox vaccine. Robert Koch came up with a method, using anthrax, to show that a pathogen caused as disease. We are not finished understanding the immune system, and probably never will be. Immunologists have adapted a complex nomenclature that is not easy to learn, as generations of medical, nursing, and graduate students have found. Still, people do learn the details and that has been immensely valuable. It would be hubris to assume that no new discoveries are in the offing.
The messenger RNA used in the vaccines we have discussed was once an abstract concept, something that had to exist but could not be seen, like dark matter. That was in the late 1950’s and early 1960’s, but the problem was solved, and we have learned to manipulate mRNA and other forms of RNA and DNA. It’s not a miracle, just hard work, imagination, time, and the money for basic science in universities and other research organizations.
Allow me another short digression: Who supports basic science research in the United States? Professor Jonathan Cole, formerly the Provost of Columbia University (and briefly my boss), wrote a book on American research universities, in which he recounted the following story: In late 1944, President Roosevelt and his science advisor, Vannevar Bush, were thinking about the US government’s vast wartime investment in basic science, from physics to antibiotics. (Bush’s book about basic science inquiry, The Endless Frontier, became a seminal text in the history of American science and industry.) When Roosevelt asked what would happen to basic science when the war ended, Bush said that without funding, it would collapse. Roosevelt decided that should not happen and that idea took hold. Fortunately, someone was taking notes.
There was a reorganization of government agencies after the Second World War, including of the military, intelligence agencies, diplomacy, and more. Sometimes lost in the bigger picture is the reorganization of science—The National Science Foundation was founded to fund basic research in 1950, and the NIH was re-organized and funded for all kinds of biological and medical research. National laboratories were founded (there are 17, run by the Department of Energy). A large amount of money was
31
dispersed to universities, much of it for basic research, which, by definition, has no immediate practical or commercial application.
If a scientist had an idea—say, to find out what Toll Receptor proteins do in fruit flies (stay with me here!), there was a way to apply to the NIH for money to test that idea and to train young scientists and undergraduates in the process. The NIH and NSF do not hand out sacks of money—the application process is rigorous, not to say terrifying to a young scientist. Most grants reward ideas produced by individuals that can be tested. Some of the titles of these projects could drive non-scientists like Senator William Proxmire mad, but the totality of ideas and clever obsessed people working in labs, gave rise to enormous advances in biology, medicine, agriculture, and the physical sciences in the United States and other countries. One of these was the discovery of the components, including the Toll Receptor Protein of the innate immune system, which 40 years ago were largely unknown.
The innate immune system is a collection of mechanisms that protects cells and animals against viruses, bacteria, fungi, amoebae, and worms; it is present in all nucleated cells. The innate system is older than the adaptive immune system, which is confined to vertebrates. Mostly it is composed of barriers, like skin or the lining of the throat and gut, but it also has unique threat sensors. (Bacteria have other mechanisms of defense, including CRISPR, which, while we have been distracted by Covid-19, has been harnessed to treat sickle cell anemia, thalassemia, and other inherited diseases.)
The innate immune system does not make antibodies or T cells and retains no memory of past infections. It limits threats and alerts the adaptive immune system about the kind of pathogens that are probing our airways, skin, or blood stream. Innate immunity is always present; it is complex, redundant, and a bit of a blunt instrument. Without it we would be at risk because a person who has never seen SARS-CoV-2 or anther novel virus will have no memory B or T cells that could defend against it.
The first Toll-like receptor was reported in 1994 by Nomura and colleagues. Flies with a mutated Toll receptor died of infection. Charles Janeway and Ruslan Medvedev at Yale and other researchers showed that a Toll-like receptor could induce an adaptive immune response in animals. Toll-like receptors warn the inducible immune system about what is coming.
The receptors have distinctive properties that are easily recognized (long stretches of the amino acid leucine) and soon there were ten, each of which recognized and responded to a specific pathogen, whether a worm, an RNA virus, a DNA virus, a gram negative bacterium, or a gram-positive species of bacteria. The Toll-like receptors were discovered (like many other things) in fruit flies, where they acquired the name Toll (I don’t know why, except that Drosophila geneticists are whimsical in their naming practices).
32
Sensors of Innate Immunity: Toll-like receptor proteins cross the membranes of immune cells to sense what invaders are outside. The perpendicular lines show the Toll-like receptor proteins, or TLR’s. TLR3 and 7 bind and detect the RNA or DNA of viruses. Other TLR molecules on the surface detect bacteria, fungi, or worms. There are proteins inside the cell that act to transfer the information detected by a TLR to turn on defensive genes. When they detect a virus, the TLR3 and TLR7 receptors activate cells to produce interferon or cytokines that in turn induce other genes, perhaps hundreds, that slow the infection.
The Toll-like receptors form the innate immune system’s antennae. They extend half in and half out of immune cells and sample the outside environment for invaders. Binding an RNA virus like SARS-CoV-2 sets the innate immune system off (it hates viral mRNA, to be anthropocentric for a moment). The Toll-like receptor TLR7 recognizes general properties of any RNA virus and signals the cell to turn on the genes involved in RNA virus defenses. They also attract defensive cells to the lung or other site of infection. This police force includes neutrophils and eosinophils that quickly arrive in the lung’s capillaries, penetrate the capillary wall, and get into the virus-infected air sacs. They accumulate quickly and attack the virus.
Imagine a lipid droplet containing thousands of Covid-19 virus particles inhaled by a victim. Those viruses can escape onto the membranes of cells in the nose, throat, or lung. The virus binds to the lung cell protein ACE2, the landing site for the Spike protein, and gets pulled into the cell. Its RNA then gets translated into new viruses. This sounds ominous and it may turn out that way, but macrophages (or cells like them) in the throat, sinuses, and lungs have also sensed the invaders. Normally they digest the virus, but they also let the body know that an RNA virus is attacking.
If there is too much activation, a so-called cytokine storm can occur and that is destructive because many of these recruited cells carry digestive enzymes that are released, causing tissue destruction and inflammation. As part of inflammation, the lung’s capillaries leak, and the air sacs fill with fluid and defensive immune cells. The process can leave a mess. Inflammation is the event that the dexamethasone (steroid) treatment and other interventions control.
33
If the innate immune system functions well in the week or two after SARS-CoV-2 infection, before the more specific B and T-cells have entered the fray in large numbers, it limits early SARS and other infections. Children have robust innate systems, according to one paper I read. Older adults have much less active innate immune systems. If so, we might ask whether the DNA of very sick Covid-19 patients contains disabling mutations in genes of the innate immune system. At least for some patients, that seems to be the case. Other vulnerable patients have antibodies against their own interferon, a critical downstream component of innate immunity.
Nature often beats us to interesting treatments. Perhaps, giving people harmless RNA will stimulate the innate immune system enough to provide protection. We need some general defense to cover the first weeks of new virus infections. Vaccines are superb instruments of medicine, but it still takes a year to make and test a vaccine and about two weeks for it to work.
Omicron, That’s Enough
What have the scientific, pharmaceutical, and medical communities done to stifle SARS CoV-2 infections since January 2020? There were (summer 2022) 18 advanced trials of different vaccines, 64 possible new treatments, and 23 potential or approved anti-viral drugs.
The mRNA vaccines from Pfizer and Moderna are robust in technology and protection. (The mRNA technology is being applied to HIV, malaria, and other diseases for which conventional vaccines have failed.) mRNA vaccines are expensive and need to be shipped frozen. Lower income countries need an effective vaccine that is inexpensive, survives at higher temperature, can be made locally, and distributed rapidly. Corbevax, created at Baylor College of Medicine, fits and is currently being made in millions of doses and distributed in India. Corbevax induces antibodies that react with proteins in addition the Spike protein. That may protect against new Spike variants. Variation in two proteins would appear much less frequently.
Beyond vaccines there are 64 new treatments (Spring 2022) that block or slow infection or some of its consequences like inflammation. Inflammation makes blood vessels leaky; defensive cells, which rush to the site of infection, squeeze out of the circulation, and infiltrate the lungs. They fill air sacs with dead neutrophils, eosinophils, and fluid, making the patient struggle to breathe. These cells release digestive enzymes that can do terrible damage to the lung or other infected tissues. Most viruses have means to inhibit a host’s immune system: some inhibit interferon synthesis, a critical mobilizer of the immune response; SARS-CoV-2 inhibits the production of Natural Killer cells, which normally recognize infected lung cells and kill them. The use of steroids to inhibit
34
inflammation was a critical early discovery. It is still the best early intervention that we have, according to a review I read recently.
There are 23 antivirals in testing or approved by the FDA, including Merck’s Molnupiravir and Pfizer’s Paxlovid, but others that have Emergency Use Authorizations as well. Paxlovid, if taken within 5 days of the onset of symptoms, blocks disease progression and keeps 90% of patients out of the hospital. That saves misery, money, and morale; it allows hospitals to function for other patients. Vaccinated and boosted people usually have a short illness and may not need these therapeutics. But for those who do, they are becoming available in pharmacies.
My friend, Jonathan Sanoff, keeps track of these things. He told me about a site called the Therapeutics Locator, which The Assistant Secretary for Preparedness and Response at The Department of Health and Human Services and her staff have prepared. The Assistant Secretary is Rear Admiral Rachel L. Levine, MD. The site tells potential patients where to find these drugs, whether in Puerto Rico or Alaska. For skeptics, the site also includes the number of doses on hand at each site and the total made so far as well as information on each drug. As new therapies come online, they will appear on the Therapeutics Locator. There are, in the summer of 2022, 7 drugs and monoclonal antibodies on the site. The Asst. Secretary and her office do not get much credit, but they should. See: https://covid-19-therapeutics-locator-dhhs.hub.arcgis.com/.
It is important to have many anti-viral drugs, and I was surprised to learn that 23 are still in late clinicals trials. Realize that this number will change. We learned from HIV therapy that an RNA virus can develop resistance to a single drug but cannot evolve resistance to three drugs and that is why the number 23 was a pleasant surprise. An even better
surprise is that some of these drugs inhibit other RNA viruses that we have covered in earlier columns, including Zika and Ebola.
Nothing in science or medicine must work, no matter how clever the idea. We should not be surprised that 26 vaccines failed, 92 treatments did not pass muster, and 54 antivirals did not inhibit SARS-CoV-2. These results on therapies in the development pipeline have been collected by Heidi Ledford, one of Nature’s senior reporters (Nature, March 3, 2022). In that context the March 11 issue of Science, the flagship publication of the American Academy of Sciences, contains a detailed comparison and analysis of these treatments and ideas on what we need to prepare for the next epidemic. Pandemics are too large a subject to cover every important event—we have slighted the value of logistics and convincing people to take vaccines, not to mention long Covid, but people are studying these challenges. The combination of basic science, private industry, and public health services has done well, even if praise sounds hollow.
What to do? Get vaccinated and boosted. When new boosters designed to attack SARS CoV-2 or other variants like Omicron appear, get those too. Even with the vaccine, you may get mild disease, but the name of the game is to prevent progression to serious
35
disease, hospitalization, or death. The new drugs should help. In places where the virus and infection are in decline, it is time to resume normal life. Or at least that is my plan.
Who Will Deal a Pandemic in 2040?
Good stories attract good students
Nothing is more valuable in the world of infectious disease than the human ability to watch for calamity coming over the horizon. That is what the CDC, the World Health Organization, various well-funded private agencies, and specialists in the Department of Agriculture do (bird flu is on the march). No organization or country is big enough to watch for all impending diseases and to do initial studies when they find one. What we really need is bright young people coming into the field. Perhaps surprisingly, most studies of infectious diseases are done by PhDs, or master’s degree level students, so an MD degree is not essential. Louis Pasteur was not a physician, but no one changed medicine more.
Graduate PhD studies in the sciences are largely tuition free and usually come with a research or teaching stipend.
The scientists and physicians who will confront a pandemic in 2040 are now in high schools around the world. Investment in people is what The United States did during and after World War II and after Sputnik—and that surely worked. There is nothing better to engage students in science and medicine than a good story. I was attracted to science by a series of elegant medical detective stories by Berton Roueché, as were many other scientists and physicians. His bell-clear stories appeared in The New Yorker beginning in the 1940’s and continued for several decades.
The first Roueché story I read was Eleven Blue Men. It begins: At about eight o’clock on Monday morning, September 25, 1944, a ragged aimless old man of eighty-two collapsed on the sidewalk on Dey Street, near the Hudson Terminal. A little further on we learn that: The old man’s nose, lips, ears, and fingers were sky-blue. Sky-blue? Not just a little blue, as in cold, but sky-blue? Really?
Soon we meet Dr. Morris Greenberg and Dr. Ottavio Pellitteri of The New York Department of Public Health—the chief epidemiologist and a field epidemiologist. Dr. Pellitteri traced the blue men to bleak Bowery hotels and then to a restaurant where they all ate. He discovered that all these men had eaten oatmeal with sodium nitrite (used to cure meat) rather than sodium chloride (table salt). Ten of them recovered and the blue color gradually faded. One succumbed to tuberculosis, then common. Berton Roueché’s stories about health detectives from the New York Health Department and the CDC are extraordinary—there is a fine anthology called The Medical Detectives. If you are a student considering nursing, science, medicine, or journalism, or if you like clear writing, read his stories. Data are not enough. We need narrative.
36
Decades after I read Eleven Blue Men, I was teaching medical and PhD students at Columbia University’s Irving Medical Center when a physician-investigator from the New York Department of Public Health called me. She needed a reference for a young researcher from my lab; he had applied for a job as a disease detective on her service. We talked for a while (he got the job) and then I asked if it was true that the Health Department’s conference room was named for Berton Roueché. She seemed delighted that I had asked. It is! He’s my hero, she said. He changed my life! We talked for a pleasant half hour. It’s good to have kindred spirits.
Mr. Roueché died in 1983, but his column in the New Yorker, Annals of Medicine goes on. CDC and the New York Health Department continued to solve cases. For example: In April 1993, a young Navaho woman on her way to a friend’s wedding in Gallup, New
Mexico developed trouble breathing. Physicians and nurses at the Gallup Indian Medical Center tried to help but she developed a devastating pneumonia and died. A week later so did her fiancé. Twenty-six people, Native American, Hispanic, and Caucasian, most of
whom were young and healthy, fell ill and thirteen died. The New Mexico Department of Public Health called the CDC.
The lungs of these patients were white with liquid that blocked X-rays. There was one clue: X-ray images looked like those from a Hantavirus patient seen years before in Korea. Hantavirus infections of humans had never been found in the United States, but the CDC scientists knew that mice carried hantavirus and reasoned that mice around the victims’ house might as well. The crawl space under and around the house turned out be full of mouse urine and feces, both with high levels of Hantavirus. When the ground dried, the wind whipped these leavings into an aerosol that the victims had inhaled. Hantavirus is not confined to the Southwest—it is ubiquitous.
I remember a seminar at Columbia University Medical Center at which a CDC investigator explained how his team had solved the case. The lecture hall seats about 150 people, and was packed with scientists and physicians, many standing in the aisles, on the sides, and the spaces at the back. When the speaker showed X-ray images of the victims’ lungs, there was a gasp; one did not have to be a radiologist to know that these people could not breathe, and that Hantavirus was the cause. The case was solved in days by trapping the mice and decontaminating the ground.
The novel Hantavirus was named Sin Nombre (no name). Sin Nombre virus is a nasty piece of work, one of our most worrisome, for which there is still no vaccine or treatment. Navaho elders had made the association between mice and pneumonia long before. CDC issues guidelines for diagnosis and provides training for physicians practicing in the Four Corners Region of the Southwest. Public health measures keep Sin Nombre at bay. Unlike SARS-CoV-2, Sin Nombre is not transmitted person to person. Fortunately.
37
The Importance of a Good Book
The Story of Molecular Biology of the Cell
Years ago, never mind how many, a biology student from Manilla wrote to me about earning a PhD. At the time, I was the Director of the PhD program in the Department of Anatomy and Cell Biology at the Columbia University Medical Center. (It is now the Columbia University Irving Medical Center, after a generous and humane donor). Every year we recruited graduate students who would spend the next five years taking courses, doing thesis research, teaching, and learning the craft of science.
An application from the Philippines was a long shot but we had enough funding to take a few foreign students. The application is arduous, containing the standard questions anyone applying to college knows about, but are more challenging. We also look for something unusual and our applicant (now a successful part of American science) had two such items in his resume. First, he had built a working replica of the first microscope made by Antonie van Leeuwenhoek in the late 17th century, and second, his essay told us there were only three copies of Molecular Biology of the Cell in the Philippines (probably an underestimate), and he owned two of them, which he had studied. We thought that showed initiative, so we interviewed him by phone and then invited him to New York where he did his thesis in my lab.
I confess I have buried the lede, which is the story of Molecular Biology of the Cell. By 1979, scientists could sequence DNA, manipulate specific genes, and had discovered that the cells of higher organisms had molecular innovations that bacterial cells lacked. Immunology advanced; cell biology, and other fields developed. These advances deserved a clearly written book for students, and frankly, for their teachers, who knew specific fields like bacterial genetics, but were vague on other areas of biology where we knew molecular biology was going to lead us. If today science can make mRNA vaccines and produce therapeutic monoclonal antibodies to control inflammation, among other practical discoveries, students and their mentors owe a debt to Molecular Biology of the Cell.
The first edition came out in 1983 from Garland Publishing, a firm with an interest in scientific textbooks. Garland was owned by Elizabeth (Libby) and Gavin Borden of New York and Norfolk Conn. The first edition was planned in Norfolk, where we live. Libby still does. The idea for a new book came from Jim Watson, the Nobel Prize winning Director of the Cold Spring Harbor Laboratories on Long Island, whose previous books, the Molecular Biology of the Gene, and The Double Helix covered an earlier period. Jim Watson and Gavin Borden knew each other and because, according to Libby, Jim thought Gavin was fun, Garland became the publisher.
38
Recruiting six excellent scientists to cover all aspects of cell and molecular biology was difficult. They had other things to do; all ran labs and taking summers to write a book was hard for them and their families, who were not allowed at writing sessions. The 1983 edition defined the style and the process of writing and editing. The diagrams and photographs were created and frequently revised as the text changed. The story of this period has been captured in a manuscript by Heather Ann Burton titled A Window on Collaboration: The Story of Molecular Biology of the Cell. It has not been published, but it is a trove of information about the authors and publishers, their personalities, tensions, and capacity for cooperation. Ms. Burton recently passed away, but her manuscript has been deposited in the archives of the Cold Spring Harbor Laboratories, a storied center of genetics and genomics on Long Island.
Elizabeth Borden in Norfolk CT, showing the first edition. The fourth edition, 2001, is behind her. The 7th edition arrived September 1, 2022.
Libby says that the first edition was difficult because the authors were creating from a blank slate. Garland had invested quite a lot of money but neither Libby nor Gavin knew
39
how many copies they would sell. Libby thought a hundred or so in the first few weeks. In the event, they sold tens of thousands. Many of the original authors, American and British, remain for the 7th edition. Bruce Alberts, a legendary biologist, and passionate supporter of science education has been the lead author from the beginning.
What made it so good? Clarity. Simple declarative sentences, excellent headings, and colored diagrams backed by images make it a joy. The book was beautifully designed. This was a relief from other texts, some of which I had fought through as an undergraduate or graduate student. The hardbound copy of the 4th edition of 2002 (1463 pages) was described by Libby as too heavy to pick up, but too interesting to put down, which is true. One of my colleagues, preparing for a lecture, held a hard copy to his chest, did twenty crunches, and then looked up muscle contraction. It’s a versatile book.
Afterword:
Vannevar Bush’s Endless Frontier did not roll west into the Pacific Ocean. The people who settled this scientific frontier explore new places with telescopes parked a million miles in space and robots and a helicopter on Mars. Or, in the tradition of Pasteur, in microbiology labs. Every time we think a simple organism like the bacterium E. coli has nothing more to tell us, someone discovers CRISPR, a way to make specific mutations.
The 3-dimensional structures of proteins can now be predicted from their amino acid sequence by the techniques of artificial intelligence. As we have seen, new antivirals have been designed to inhibit lethal viruses. There is still a lot that we do not know about Covid-19 and thousands of other viruses. Their multitudes can still overwhelm our chemists, biologists, physicians, and computers, but eventually we catch up. We must learn to do it faster.
If we are thinking about complexity, studying communities, whether wasps and ants or the bacteria of the gut microbiome, there are problems to be solved. Who knew, for example that the gut pathogen, Vibrio cholerae has a way to kill other bacteria that compete with it in the gut? There are thousands of stories like that waiting to be uncovered.
Scientists did not anticipate how vaccines enrage people who do not believe in vaccination and understandably, do not want to give up the control of their own bodies. It should be voluntary, they believe, and that is reasonable, but infectious disease does
40
not play by democratic principles. An infected, unvaccinated person sustains the disease. There is nothing I can think of to change that anti-vaccine attitude except patience and education.
Sources and Other Light Reading
The Plague Year by Lawrence Wright, The New Yorker, Jan. 5, 2021. Now a book. Rage by Bob Woodward 2020. Simon and Schuster, (unique sources, as usual) CDC: https://www.coronavirus.gov
NIH: https://www.nih.gov/coronavirus
NCBI SARS-CoV-2 literature, sequence, and clinical
content: https://www.ncbi.nlm.nih.gov/sars-cov-2/
The Therapeutics Locator: https://covid-19-therapeutics-locator-dhhs.hub.arcgis.com/
This Week in Virology, TWIV. A podcast by Professor Vincent Racaniello and colleagues. It covers all of virology in detail, including therapeutics.
How The Immune System Works; 5th edition. Lauren Sampayrac, Wiley Blackwell, 2016 Molecular Biology of the Cell, 7th edition. September 2022. Available from Norton Press.
Silent Invasion: The Untold Story of the Trump Administration, Covid-19 and Preventing the Next Pandemic Before it is Too Late. Dr. Deborah Birx. HarperCollins, 2022.
The Famine of Men, 2014, a novel about a young virologist trying to establish her first lab. The book is about how science works and the people who do it. By chance, our protagonist discovers a virus that kills Leydig cells, which produce testosterone. The virus is incredibly infectious, and, despite serious efforts, vaccines have failed. There are consequences—lots of them. By the author, who tired of scientific prose. From AuthorHouse.com or Amazon.com.
41
The phrase, ‘World Enough and Time’, used on page 12 to describe the potential for mutation in viruses, was borrowed from Sir Andrew Marvel’s poem To His Coy Mistress. Sir Andrew was a 17th century English poet and rake.
‘Waiting it the Hardest Part’, Page 12, is a lyric by the incomparable Linda Ronstadt.
Relevant Columns from The Body Scientific in The Lakeville Journal: See Richardkessin.com for thoughts on other subjects. The website has functional links.
For all Body Scientific Columns see:
The Coalition for Epidemic Preparedness Innovations: Progress has been made on Ebola and other diseases
Part 1 of 2 In 2014 and 2015, Ebola virus infection killed 8,698 people in Sierra Leone, 3,337 in Guinea and 3,955 in Liberia. There were survivors… 03/14/2016
09/13/2017
Ebola, Ça suffit! (Ebola, that’s enough!): Progress has been made on Ebola and other diseases
Part 2 of 2 Ebola virus periodically leaps out of a reservoir in Africa and causes high mortality in humans and great apes. We do not know for sure…
The Ebola threat: What we learned from it
We learned that some people panic, and others do not. We learned that physicians, nurses, hospitals, the CDC and the NIH make mistakes, but we have…
09/06/2017
How a rabies vaccine captured the public’s imagination in 1885 02/17/2016
Control of Infection: The Germ Theory of Disease was a liberating idea that helped extract medicine from near futility.
04/24/2015
When conviction trumps evidence: Lessons of a measles outbreak
42
Before 1963, almost all children got measles in the United States. Decades later some remember it as a rite of passage, unpleasant certainly, but not 04/16/2015
Elie Metchnikoff, World War I and the End of Optimism
We observe the end of World War I on Nov. 11, Armistice Day. For Americans, World War II is the more remembered event, but the calamity of World War I…
10/17/2014
What story does the DNA tell us?
When I was a Ph.D. student in the late 1960s, a scientist determined the exact DNA sequence that encoded the plan for part of a protein. He and his team sequenced 23 nucleotides. It was a triumph…
01/30/2012
08/16/2011
Epidemic remembered
In 1735, a diphtheria epidemic swept through Connecticut and the rest of New England. It started in Princeton, N.J., and raged up the coast for several…
43